• To increase your understanding of a variety of leadership models
• To recognise the core elements of effective ward leadership
• To contribute towards revalidation as part of your 35 hours of CPD (UK readers)
• To contribute towards your professional development and local registration renewal requirements (non-UK readers)
Nurses who are responsible for a clinical area do not only have a management role but also, crucially, a leadership role. The role of ward leader is complex and demanding. Ward leaders are accountable for patient safety and the quality of patient care, act as role models, motivate staff and cascade organisational goals to them. They also ensure the correct skill mix on the ward, alleviate pressures on staff and provide opportunities for staff development. This article describes several leadership models which all have something to offer to nurses looking to develop their ward leadership skills. It discusses core elements of effective ward leadership, notably providing support and direction to the team through coaching and mentoring, developing the ward as a learning environment, understanding the wider care context and taking time for self-care.
Nursing Management. doi: 10.7748/nm.2023.e2043
Peer reviewThis article has been subject to external double-blind peer review and checked for plagiarism using automated software
Correspondence Conflict of interestNone declared
Richards A (2023) Developing ward leadership skills. Nursing Management. doi: 10.7748/nm.2023.e2043
Published online: 04 April 2023
This article aims to support nurses who lead a clinical area to better understand the leadership models that may help them in their role and reflect on some of the core elements of effective ward leadership. After reading this article and completing the time out activities you should be able to:
• Understand the principles of transformational leadership, situational leadership, authentic leadership and compassionate leadership.
• Describe how each of these leadership styles can support effective ward leadership.
• Explain how ward leaders can provide direction and support to their team through coaching and mentoring.
• Characterise the role of ward leaders in developing the ward as a learning environment.
• Recognise the need for ward leaders to understand the wider care context and develop a self-care plan.
Optimal leadership at ward level is essential for the effective functioning of healthcare organisations and for improved patient safety, outcomes and experience (Whitby 2018). The Francis (2013) report and Berwick (2013) report outlined the harmful consequences which diffuse leadership, with unclear roles and lack of ownership, can have on patient care. Optimal ward leadership is more important than ever in today’s acute healthcare settings, where the focus is on maintaining the quality of patient care and ensuring patient safety while managing staff fatigue in the wake of the coronavirus disease 2019 (COVID-19) pandemic.
In their leadership role, ward managers need to take ownership for what occurs at ward level and act as role models for staff. The role of ward leader involves being accountable for patient safety and the quality of patient care, as well as motivating staff, fostering work engagement and cascading organisational goals. The role is also crucial to the implementation of evidence-based care (Bianchi et al 2018). Other aspects of the role of ward leader include ensuring the correct skill mix on the ward and retaining staff, particularly given the global shortage of nurses and unfilled vacancies in clinical areas (The Health Foundation et al 2018), which require them to alleviate workload pressures on staff and provide them with opportunities for professional development. In its Nursing Workforce Standards – which set out what needs to happen in workplaces to ensure safe and effective patient care – the Royal College of Nursing (RCN) (2021) highlights the important role of nurses with lead clinical professional responsibility in workforce planning and professional development.
Read the RCN’s Nursing Workforce Standards at: www.rcn.org.uk/professional-development/publications/rcn-workforce-standards-uk-pub-009681. Which standards are relevant and/or central to your role? How would you uphold these in practice? Write down your reflections and discuss these with your team at the next team meeting
There is no recognised ‘right’ leadership style or model which suits every situation (Maxwell 2017). Nurses in leadership positions, including ward managers, face numerous demands and challenges, so they need to be knowledgeable about leadership styles and be able to use the most appropriate approach according to the situation. Leadership styles that can be used to support optimal ward leadership include transformational leadership, situational leadership, authentic leadership and compassionate leadership.
• Ward leaders need to be knowledgeable about leadership styles and be able to use the most appropriate according to the situation
• Ward leaders can use coaching and mentoring to provide direction and support to the team
• Ward leaders need to create an environment conducive to learning where members of the team support each other
• Clarity about the organisation’s direction can enhance ward leadership
• Ward leaders need protected time to look after their own well-being
The Nursing and Midwifery Council (2018) considers leadership to be an essential component of the nurse’s role and describes nurse leaders as role models. Being a role model is a central element of leading a team, and for that purpose transformational leadership may be the most relevant style to adopt. Transformational leadership, as outlined by Burns (1978), is a high-impact style of leadership which sets a shared vision, empowers followers and gives them a sense of purpose (Fischer 2016). Bass and Avolio (1994) described transformational leadership as being at one end of a continuum, with transactional leadership styles in the middle and laissez-faire leadership at the other end.
Northouse (2021) described leadership in terms of followers being influenced by leaders to work towards a single goal. While motivating followers and articulating clear goals and expectations can be considered elements of traditional leadership styles, they also feature in transformational and transactional leadership. In contrast, authors such as Drath (2008) and Hulks et al (2017) outlined a style of leadership which is about dialogue and working across boundaries to foster participative and facilitative ways of working. Ward leaders generally need to be able to work across boundaries to navigate the healthcare system and manage its complexities.
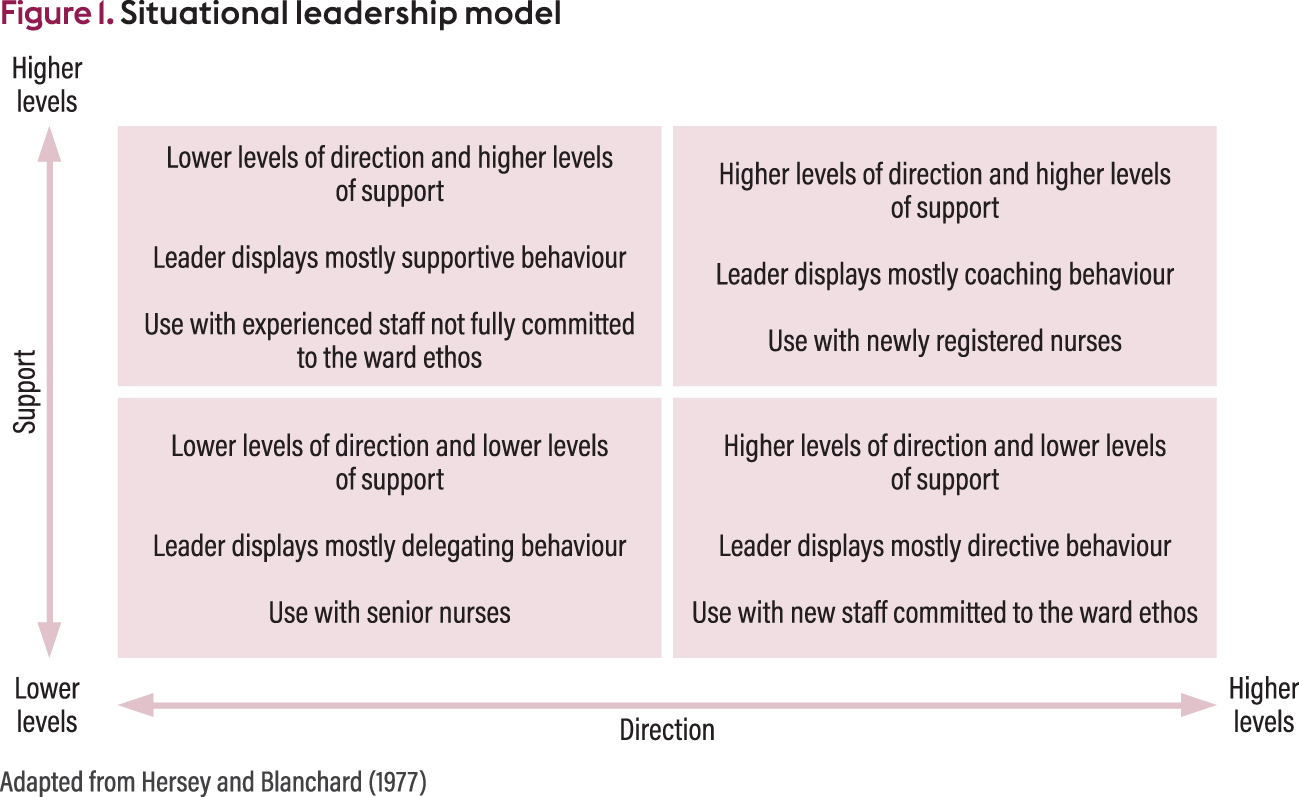
Situational leadership, one of the most accessible leadership models for ward leaders, was first described by Hersey and Blanchard (1977). It was used for national leadership programmes rolled out to ward leaders in the early 2000s – such as the RCN Clinical Leadership programme (www.rcn.org.uk/professional-development/professional-services/leadership-programmes/clinical-leadership-programme) and the Leading an Empowered Organization (LEO) programme (Jones 2005) – and is still widely used to teach leadership skills to ward leaders.
The original situational leadership model was revised and updated by Blanchard et al (2010), but it is still based on the leader tailoring the amount of direction and support they provide to the follower according to the follower’s confidence, competence, experience and commitment. The situational leader will display a finely tuned mix of directive, supportive, delegating and/or coaching behaviours to match the direction and support needs of each member of staff. For example, a newly registered nurse may need coaching, which requires higher levels of direction and support, while a more senior nurse may require delegating, which requires lower levels of direction and support. Staff who are committed to the ward ethos but lack experience may need lower levels of support but higher levels of direction, while staff who are not fully committed to the ward ethos but have extensive experience may require lower levels of direction but higher levels of support (Hersey and Blanchard 1977, Blanchard et al 2010).
Figure 1 illustrates the situational leadership model.
Situational leadership has been criticised because it requires leaders to alter their behaviours, which Thompson and Glasø (2018) believe is difficult or even impossible – or at least unsuitable – and because there is little empirical evidence of its value (Vecchio 1987, Thompson and Glasø 2018). There has also been criticism that, considering its widespread use, the situational leadership model has not been sufficiently researched or tested (Thompson and Glasø 2018).
However, adopting a fluid leadership style that gives each member of the team what they need is probably reasonable for a ward leader. Each team member is an individual with unique needs. Encouraging their development involves using a leadership style that matches the support they require, and ensuring every team member is supported to enhance their skills and confidence will lead to better outcomes for patients (Lyubovnikova et al 2017).
Considering leadership in the context of inclusivity and compassion is something ward leaders should find attractive, particularly since clinical areas continue to be negatively affected by the unprecedented changes brought about by the COVID-19 pandemic. Those changes combined with chronic nurse shortages mean that healthcare organisations need inclusive and compassionate ward leaders.
In a discussion of authentic leadership – which was first described by Avolio et al (2004) – Alilyyani et al (2018) focused on the need for the authentic leader to behave ethically and display integrity to create a climate of openness and trust, something that is very much needed at present. Authentic leaders are self-aware and transparent. They present as who they truly are, which creates a climate of openness and trust. Others can see the person behind the role and mirror their behaviour. Authentic leadership is believed to encourage learning, thereby decreasing errors (Farnese et al 2019) and enhancing patient safety.
Using an authentic leadership approach to ward leadership has been shown to contribute to engaging nurses in their work (Bamford et al 2013). Nurses with high work engagement find their work fulfilling, are enthusiastic about and dedicated to what they do, and contribute to the organisation (Cai et al 2021). With a global shortage of nearly six million nurses (World Health Organization 2020), it is essential that ward leaders invest time and energy in cultivating work engagement among staff.
The benefits of compassionate leadership for health and social care, first described by West (2021), are being increasingly recognised. The Nursing Workforce Standards (RCN 2021) suggested that ‘nursing leadership must embody compassion both in style and behaviour towards the staff they lead’. West (2021) stated that compassionate leadership, characterised by humanity and presence, makes a significant difference to staff and patients. Its benefits include protecting everyone’s well-being and reducing the risk of medical errors (West 2021). Compassionate leadership is a collective leadership where leaders work together within and outside their organisations to discuss issues and foster supportive networks (West 2021). West (2021) outlined four core behaviours required of compassionate leaders: attending, understanding, empathising and helping. Box 1 explains what these four core behaviours require of ward leaders.
Attending
For ward leaders, ‘attending’ requires being present in their clinical area and listening to others. This enables them to develop a good ‘understanding’ of what is going on for staff, their needs and perspectives – which sometimes conflict with the leader’s needs and perspectives
Understanding
For ward leaders, ‘understanding’ requires having a good grasp of the daily issues that affect the ward and the wider issues that impinge on care quality and patient safety. It also requires being open to difference
Empathising
For ward leaders, ‘empathising’ requires the ability to appreciate and relate to the feelings and experiences of others without becoming overwhelmed – self-care is critical to one’s ability to empathise
Helping
For ward leaders, ‘helping’ requires taking action and being seen to take action, removing obstacles to success and providing staff with the resources they need to do their job
(Adapted from West 2021)
The article now focuses on five core elements of effective ward leadership:
• Combining management and leadership roles.
• Providing coaching and mentoring.
• Creating a learning environment.
• Understanding the wider care context.
• Looking after oneself.
The role of ward leader is complex and far-reaching, and there are important considerations as to how leadership should be applied at ward level. Ensuring staff comply with policies and procedures can sometimes feel at odds with providing direction and support to the team. Implementing policies and procedures while inspiring staff to work towards organisational goals requires a nuanced approach which combines management and leadership. Neither management nor leadership should dominate the ward leader’s behaviour. Table 1 summarises outcomes that can be achieved when combining management and leadership roles (these examples are based on the author’s experience).
The ward leader can use coaching and mentoring to provide direction and support to the team. There is crossover between the two, which can lead to confusion.
A mentor’s role is supportive and educational while a coach’s role is to draw out the coachee’s skills (Viera 2021). In a mentoring relationship, the mentor is usually a senior member of staff and the mentee a junior member of staff. A mentor may go further than a coach in areas such as sharing their experiences and supporting the mentee to overcome the challenges of their role. Mentorship is widely used to encourage and support nursing students and newly registered nurses.
In coaching, there is usually no hierarchical relationship between the coach and the coachee (Viera 2021). Coaching is concerned with exploring and challenging the values, beliefs and assumptions that underpin individual behaviour and with reinforcing the person’s self-confidence and self-belief. For coaching to work, there must be an innate belief that the coachee already possesses the knowledge and skills required for clinical practice but needs support to recognise this (Viera 2021).
It is important to consider each person’s individual situation before deciding whether to use mentoring or coaching. For example, a newly appointed ward leader may benefit from being mentored by an experienced colleague, who will help them understand their new role and discuss with them matters they are unsure about (Jacobs 2018). An experienced nurse who wants to progress in their career may benefit from being coached by a colleague from another organisation who has expertise in networking or education and will help them explore the possibilities open to them, reflect on their strengths and abilities, and enhance their self-belief and self-confidence (Atkinson et al 2022).
Identify a member of your team who may be ready for promotion and could benefit from support to achieve their career development goals. What leadership style would you use to support them? Would you suggest that they receive mentoring or coaching? Would you support them yourself or ask someone else to do so?
Royal College of Nursing clinical leadership programme
Royal College of Nursing advice on well-being, self-care and resilience
www.rcn.org.uk/library/subject-guides/Wellbeing-Self-Care-and-Resilience
To motivate and inspire the team, the ward needs to become a learning environment. Developing the ward as a learning environment can lead to improved staff engagement, enhanced learning from near misses and errors, and ultimately better patient outcomes (Tomietto et al 2016). It may also lead to fewer staff absences and improved staff retention. Tomietto et al (2016) found that a clinical area where staff displayed high work engagement enhanced both student and staff learning.
The ward leader needs to create an environment conducive to learning where members of the team naturally support each other, which will enhance the atmosphere on the ward. Encouraging team members to mentor or coach others will also ensure that the team feels valued and engaged while developing leadership skills for the future.
Nursing students are often best supported to learn through mentoring, including peer-to-peer mentoring between a senior and junior student. Peer-to-peer mentoring is one form of mentoring recommended in the Collaborative Learning in Practice (CLiP) model (Health Education England 2017, Williamson et al 2020), which was implemented following issues raised by nursing students in the National Student Survey on mentorship and the availability of mentors on clinical placements (Higher Education Funding Council for England 2007). In the CLiP model, registered nurses are regarded as coaches rather than mentors, while continuing to provide student supervision, and coaching is seen as short term and skill specific, while nursing students from different years, who are all working on the same ward, act as mentors for each other (Clarke et al 2018).
Newly registered nurses can be supported and guided by more experienced colleagues to adapt to professional life and its challenges. Mentoring and coaching can be useful tools for ensuring that newly registered nurses can apply the knowledge and skills gained during their time as students to practise more effectively. If newly registered nurses are not supported, they are more likely to question their career choice (Wray et al 2021). This particularly applies to nurses from countries outside the UK who, without adequate support, may quickly feel lonely, anxious and homesick in a new system of care and a new culture (Afriyie 2020).
Senior team members can help develop the confidence of junior members by demonstrating clinical skills. For experienced nurses, being able to pass on their experience to others can be deeply satisfying and give them a sense of pride. They can also help junior members of the team to develop their ability to delegate, which is a measure of a safe and effective clinical environment and a fundamental skill newly registered nurses may lack (Balluck 2022, Crevacore et al 2022).
Two overall goals of most healthcare organisations are to achieve optimal patient outcomes and well-performing, safe clinical areas. However, what is driving one specific organisation may not always be clear for ward leaders. In a study in Denmark, Hølge-Hazelton et al (2021) found that a lack of insight into organisational goals resulted in ward leaders lacking belief in their own role – other contributing factors were suboptimal communication within the hierarchical structure and difficulties balancing competing needs. Clarity about the organisation’s direction and the motivations of people in senior leadership positions can enable clinical areas to work in a strategic way, rather than troubleshoot and firefight. It can also enhance ward leadership in times of crisis, such as the COVID-19 pandemic (Hølge-Hazelton et al 2021).
While ward leaders usually have financial and budgetary responsibilities, these are often limited in scope and ward leaders do not always have the level of budgetary control they would wish for. Furthermore, resources for their ward may not be as generous as they would like, so it is important for ward leaders to understand the wider financial and budgetary context in which resources are allocated.
Ward leaders also need to be aware of the latest recommendations issued to their organisation by the Care Quality Commission and prepare for scrutiny of their clinical area. Many wards seek to join internal and/or external accreditation programmes and some healthcare organisations conduct small-scale inspections to check their preparedness. Understanding the regulatory framework and quality assurance processes, and what they mean for the clinical area and the team, is a crucial part of the ward leader’s role (Siegel et al 2018, Hope 2022).
It is also important that ward leaders are aware of the wider context in which their organisation operates and of changes at national level that will affect their organisation. For example, ward leaders need to be aware of the direction set by the Department of Health and Social Care (2021) in its white paper entitled Integration and Innovation: Working Together to Improve Health and Social Care for All. An understanding of wider issues affecting the NHS, such as the continuing effects of the COVID-19 pandemic, waiting lists and winter pressures, is also useful.
How much time do you dedicate to self-care? Do you have a self-care plan? If not, take this opportunity to draft your ideal self-care plan. Do you find it challenging to follow your self-care plan? If so, think about how you could better adhere to it. Discuss this with your clinical supervisor or with a colleague who has the same level of responsibility as you at the next opportunity
Ward leaders have a stressful and demanding role which can lead to ill-health and burnout. Therefore it is important that they have protected time dedicated to looking after their own well-being. Brand et al (2017) discussed five steps towards a healthier and more engaged workforce, one of which being to develop a self-care plan. Developing a self-care plan and showing compassion to oneself – which is a prerequisite for showing compassion to others – is important. West (2021) explained that self-compassion is a central component of working towards becoming a compassionate leader. To enhance their well-being, ward leaders can source support from formal and informal networks, including from a mentor within or outside the organisation. Using a mindfulness app could be useful to reduce levels of stress in demanding situations (Xu et al 2021).
Ward leaders’ job satisfaction is often neglected, with the focus being on them juggling competing demands and tasks (Pegram et al 2015). Job satisfaction is increasingly seen as important in developing optimal ward leadership that contributes to the success of healthcare organisations (McSherry and Pearce 2016). Ward leaders may gain job satisfaction from being given clear and focused goals, the achievement of which may be assessed against systematic measures of success such as those used in ward accreditation programmes (Arun et al 2020).
The role of ward leader is crucial to the functioning of healthcare organisations and the provision of high-quality, safe patient care. Ward leaders need to combine management and leadership in equal measures and be able to use different leadership styles – such as transformational leadership, situational leadership, authentic leadership and compassionate leadership – according to the task at hand. Ward leaders also need to understand and communicate the organisations’ goals, support and motivate different members of the team through coaching and mentoring, act as a role model for the team and be compassionate and supportive while ensuring staff adhere to policies and procedures. The role of ward leader is highly demanding, so it is important that they take time for self-care.
Identify how developing ward leadership skills applies to your practice and the requirements of your regulatory body
Now that you have completed the article, reflect on your practice in this area and consider writing a reflective account. See: rcni.com/reflective-account

04 April 2024 / Vol 31 issue 2
Views of specialist head and neck nurses about changes in their role
The Cancer Reform Strategy (Department of Health 2007)...
The role of lung cancer nurse specialists
A report published by the National Lung Cancer Forum for...
Management of patients with low-risk febrile neutropenia
The National Institute for Health and Care Excellence in the...
Taking the lead and extending the role of lung cancer clinical nurse specialist
Leadership is central to the delivery and continuous...
Managing and leading educational initiatives in response to the Cancer Plan
With the advent of the Cancer Plan (DH 2000a) the...